All published articles of this journal are available on ScienceDirect.

Predictors of Difficult Tracheal Intubation on Adult Elective Patients in a Teaching Hospital
Abstract
Background:
During routine preoperative assessment of patients one of the commonest practices is predicting difficulty of tracheal intubation from various factors detected. Whether the factors reliably predict the difficulty is subject of argument. This study was conducted to assess the predictors of difficult tracheal intubation in adult patients.
Methods:
In this prospective observational study, we studied 120 consecutive elective adult patients admitted for general, gynecologic and orthopedic surgeries. Socio-demographic parameters and test variables such as BMI, TMD, SMD, IIG and Mallampati class were collected during preoperative evaluation. CL grade and difficulty of intubation were observed while the anesthetist in duty performs the laryngoscopy. While the former obtained from the preoperative anesthesia note, the latter were filled to questionnaire based on what the anesthetist reports during or after laryngoscopy. The prevalence of difficult intubation and the sensitivity, specificity, PPV and NPV of the tests were analyzed. SPSS-20 and different formulas were used during analysis. Chi square test was used and P<0.05 was considered as statistically significant.
Result:
The overall prevalence of difficult tracheal intubation was 2.5%. The sensitivity, specificity, PPV & NPV of the tests were 0%, 98.3%, 0% & 97.46% for BMI; 0%, 97.5%, 0% & 100% for SMD; 100%, 96.64%, 20% & 100% for TMD; 0%, 99.17%, 0%, & 100% for IIG; and 100%, 99.14%, 75% & 100% for Mallampati test.
Conclusion:
The incidence is not quite small that anesthetists should use necessary tests to predict the difficult intubation. Probably combining the tests being the best option, Mallampati test alone can predict the difficult intubation in adult patients.
INTRODUCTION
Difficult airway, whether anticipated or not, is a devastating event that anesthesia team encounters in perioperative care. As the brain sustains only few minutes without oxygen, delay or inability to manage the difficult airway may cause brain damage or death. Failure to manage difficult airway is reported to account for as high as 30% of anesthesia related deaths [1, 2]. Difficult tracheal intubation is one of the two distinct scenarios that determines difficult airway. The incidence of difficult tracheal intubation after direct laryngoscopy in normal patients is as high as 5.8% [3].
There are inter-individual variation of airway parameters and clinical factors. Around 12% [4] and 1.1% [5] of population is obese globally and in Ethiopia, respectively. Obesity affects neck movement during intubation. Patients with short neck are also challenging during airway management because of difficult neck extension and laryngoscope placement. Maximum mouth opening also determines the easiness of airway management and endotracheal intubation. Similarly, the distances from mandible to sternum or thyroid cartilage also have impact on easiness of placement of endotracheal tube following direct laryngoscopy.
Simple bed side patient evaluation can minimize anesthesia related airway morbidity and mortality. For this very reason, the identification of the patient with difficult airway is vital in the preoperative evaluation and planning anesthetic management, so that endotracheal intubation and positive pressure ventilation can be achieved safely by alternative methods of tracheal intubation like fibreoptic bronchoscopy. Regardless of their sensitivity and specificity, predicting factors used in reports include, but not limited to, body mass index (BMI), Sternomental distance (SMD), Thyromental distance (TMD), Interincisor gap (IIG) and Mallampati class, head and movement [6]. Combination of more than two parameters predicts expected difficulty better than using single factor. None of these tests are perfect indicator of difficult intubation [7]. However, in patients with neck mass a single factor can be significant predictor of difficult intubation [8]. Accurate preoperative prediction of potential difficulty of intubation can help reduce the incidence of catastrophic complications by alerting anesthesia personnel to take additional precautions prior to anesthesia and establishing an artificial airway. Furthermore, more accurate prediction of difficulty of intubation might reduce the frequency of unnecessary maneuvers (e.g. awake intubation). However, it is still questioned whether accurate prediction is possible and which variables should reliably be used for evaluation [9].
This study, therefore, assesses the prevalence and predicting factors of difficult intubation among adult patients who undergo major surgeries under general anesthesia with endotracheal intubation.
METHODS
After obtaining approval letter from the ethical committee, 120 consecutive adult patients for major elective surgeries, in Jimma University teaching hospital (JUTH), were included in the study. Prospective observational study design was employed. The study was conducted from January 2012 to May 2012. Patients with ASA III&IV, need for rapid sequence induction, pathologic condition in the airway and unwilling patients to participate were excluded from the study. All patients were elective patients scheduled for gynecologic, orthopedic and general surgeries.

During preoperative visit at bed side or in pre induction room, socio-demographic characters and risk factors for difficult intubation were assessed. During intubation the data collector documented the events attributed to laryngoscopy and endotracheal intubation based on the feedback from the anesthetist on duty. Difficult intubation is defined as difficulty to properly insert tracheal tube in three attempts or within 10 minute with conventional laryngoscopy [10]. During preoperative assessment, sex, age, BMI, SMD, TMD, IIG and Mallampati class were documented. BMI > 30kg/m2 was used as obese. SMD measured with tape and categorized SMD< 12cm and greater than 12cm. likewise, TMD was categorized as TMD < 6.5cm and greater than 6.5cm. IIG was categorized as IIG< 3cm and greater than 3cm. Malampati class was also assessed and classified as follows: class-I when soft palate, fauces, uvula & pillar seen, class-II when soft palate, fauces & uvula seen, class-III when soft palate & base of uvula seen and class-IV when soft palate not visualized (Fig. 1). Based on laryngoscopy, CL laryngoscopy grade was as follows: grade-I when part of vocal cord was visible, grade-II when only the arytenoids were visible, grade-III when only epiglottis was visible and grade-IV when epiglottis was not visible (Fig. 1).
Before analysis the data was cross-checked for completeness and consistency. SPSS-20 was used to analyze the data. Except the age of the patient for which we use student’s t-test, chi-square test was used. P< 0.05 was considered as statistically significant. The sensitivity, specificity, positive predictive value and negative predictive values were computed using standard formula
Sensitivity= Number of accurately predicted difficult intubations ÷ Number of difficult intubations encountered
Specificity= Number of accurately predicted easy intubations ÷ Number of easy intubations encountered
PPV= Number of accurately predicted difficult intubations ÷ Total number of intubations anticipated to be difficult
NPV= Number of accurately predicted easy intubations ÷ Total number of intubations anticipated to be easy.
RESULT
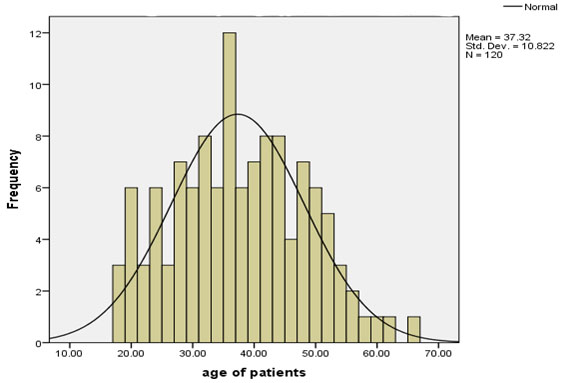
160 consecutive adult patients scheduled for elective surgery under general anesthesia with endotracheal intubation were selected and 120 of them fulfilled the inclusion criteria and employed in this study. 81(67.5%) male and 39(32.5%) female patients participated in the study (Table 1). The age of the patients in Mean+ SD was 37.3+10.8 years (Fig. 2).
| Variables |
Frequency (n) |
Percentage (%) |
Difficulty of TI Easy(n) Difficult(n) |
|---|---|---|---|
| Sex: Male Female |
81 39 |
67.5 32.5 |
79 2 38 1 |
| BMI: < 25kg/m2 ≥ 25kg/m2 |
118 2 |
98.3 1.7 |
115 3 2 0 |
| Type of surgery: Orthopedic Gynecologic General |
20 18 82 |
16.7 15 68.3 |
19 1 17 0 81 2 |
| TMD: ≤ 6.5cm > 6.5cm |
5 115 |
4.2 95.8 |
4 1 113 2 |
| SMD: ≤ 12cm > 12cm |
3 117 |
2.5 97.5 |
3 0 115 3 |
| IIG: ≤ 3cm > 3cm |
1 119 |
0.8 99.2 |
1 0 116 3 |
| Malampati class: I&II III&IV |
116 4 |
96.7 3.3 |
116 0 1 3 |
Out of 120 patients; 20 underwent orthopedic surgeries, 18 gynecologic surgeries and 82 general surgeries. 118 patients had BMI < 25kg/m2 out of which 3 were difficult to intubate yet with no statistical significance and 2 patients had BMI > 25kg/m2 but both were easy to intubate. 5(4.2%) patients had TMD < 6.5cm of whom 4 had easy and 1 had difficult intubation (p<0.05), whereas the rest 115 (95.8%) had TMD > 6.5cm and only two of them were difficult to intubate. 117(97.5%) and 3(2.5%) patients had SMD >12cm and SMD <12cm, respectively but the three difficult to intubate patients were from SMD >12cm group. 119(99.2%) and 1(0.8%) patients had IIG >3cm and <3cm, respectively and all of the latter group were easily intubated. Out of 116(96.7%) Mallampati class-I&II patients only 1(0.8%) case of difficult intubation was observed but out of 4(3.3%) patients who exhibited Mallampati class-III&IV, difficult intubation was encountered in 3 patients who also were CL laryngoscope grade-III&IV which is highly significant within the group(p<0.05).
DISCUSSION
In current study we found that the incidence of difficult tracheal intubation after direct laryngoscopy was 2.5% which is almost similar to report by Aftab S et al. where the incidence was 2.6% [11]. There is a possibility of higher incidence of difficult intubation on similar patients according to varies previous studies. In a systematic review of thirty five studies, Shiga T et al. reported the overall incidence of difficult intubation on apparently healthy patients as 5.8% [3]. With this much incidence, anyone in the field of anesthesiology should expect difficult airway due to difficult tracheal intubation so as to prepare for alternative techniques. There are several strategies and algorithms to manage the airway once difficulty is anticipated [12-14]. Of all difficult intubations encountered, none of them had failed intubation.
Among the five simple bed side difficult intubation tests we used for this study, only thyromental distance (TMD<6.5cm) and Mallampati classification (class III&IV) showed significant predictive values. This finding contradicts with a report by Savva D et al. where Mallampati class, if used as a single test, found to be not a predictor of difficult intubation [15]. Both SMD and IIG had undefined sensitivity, relatively high specificity yet zero PPV. However, except for the BMI, NPV value of all tests was 100%.
In our study BMI greater than 25kg/m2 is found to be poor predictor of difficult intubation especially in detecting the true positives. The sensitivity, specificity, PPV and NPV of BMI were 0, 98.30%, 0 and 97.46%, respectively. These values are almost similar to the pervious study in which the sensitivity, specificity, PPV and NPV were 7%, 94%, 6% and 95%, respectively [16].
The sensitivity, specificity, PPV and NPV of Mallampati score were 100%, 99.12%, 75% and, 100%. This test is good indicator of difficult intubation in our study. This finding is almost in line with findings in a study on Kashmir population. AK Gupta et al. conducted a study on Kashmir population regarding predictors of difficult intubation and reported the sensitivity, specificity, PPV and NPV of Mallampati class as 77.3%, 98.2%, 48.7% and 99.5%, respectively [17]. Moreover, George and Jacob reported 54.5% sensitivity of Mallampati class as a predictor of difficult tracheal intubation [18]. TMD, although, has good sensitivity, specificity and NPV (Table 2), its PPV is very low (20%). Low PPV indicates the test’s failure to answer the anesthetist’s question regarding how likely would be the difficult intubation given that the test result was positive.
| Tests | Sensitivity | Specificity | Positive predictive value (PPV) | Negative predictive value (NPV) |
|---|---|---|---|---|
| BMI | 0.00% | 98.30% | 0.00% | 97.46% |
| SMD | _ | 97.5% | 0% | 100% |
| TMD | 100% | 96.64% | 20% | 100% |
| IIG | _ | 99.17% | 0% | 100 |
| Mallampati class | 100% | 99.14% | 75.00% | 100% |
LIMITATION OF THE STUDY
The study included all consecutive elective surgical patients who fulfilled inclusion criteria without randomization. It neither did employ power formula for sample size determination nor randomized subjects to different comparable groups. We did not analyze the correlation between CL laryngoscope grade and difficult intubation. These can be considered as limitation.
CONCLUSION
Based on the result, we conclude that the incidence of difficult intubation is not quite small that the anesthetists should expect difficult airway management in apparently normal patients. Moreover, not all preoperative screening tests reliably indicate difficult intubation when used alone. Combination of some tests may have favorable effect in predicting true difficulty. However, Mallampati class III&IV alone can predict the probability of difficult endotracheal intubation in adult patients.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

