All published articles of this journal are available on ScienceDirect.

Thoracolumbar Interfascial Plane Block (TLIP) Modified Technique for Lumbar Decompression Surgery in Cirrhotic Hepatic Patients with Thrombocytopenia: A Case Report
Authors Info & Affiliations
Abstract
Introduction:
As one of the top ranks in the pain-producing procedure, spinal surgery requires adequate perioperative pain management to improve outcomes. Likewise, perioperative pain management in cirrhotic hepatic thrombocytopenia patients is challenging. Modified TLIP block can be an option for perioperative pain management in the lumbar decompression surgery for a cirrhotic hepatic patient with thrombocytopenia.
Case Presentation:
A man, 67 years old, who suffered from cirrhosis hepatic with thrombocytopenia underwent endoscopic spinal decompression with laminotomy and flavectomy of L4-L5. After induction of general anesthesia with midazolam 1,5 mg, fentanyl 150 mcg, propofol 100 mg, and rocuronium 1mg/kg, the patient was intubated. The lungs were ventilated with a pressure control mode with tidal volume 8 ml/kg BW, respiratory rate 12/min, and PEEP 5 cm H2O with FiO2 50%. and 1% sevoflurane. Modified TLIP block was performed at the L3 level. Twenty ml of bupivacaine 0,5% was administered between the longissimus and iliocostalis muscles on both sides.
Results:
Intraoperative, modified TLIP block provide adequate analgesia with stable hemodynamics. The visual Analog Scale (VAS) of pain was 1-2 in 24h postoperative. No additional opioid was required within 24 hours postoperatively. There were no neurological complications or bleeding due to the modified TLIP block found in this patient.
Conclusion:
Modified TLIP block can be an effective and safe analgesic technique for hepatic cirrhosis patients with thrombocytopenia. However, further research is needed to determine the safety limits of modified TLIP block in patients with coagulation disorder or anticoagulant use.
1. INTRODUCTION
Spinal surgery is included in the top 6 pain-producing procedures, so adequate pain management is required to improve outcomes [1, 2]. The best approach for pain control is combination therapy or multimodal analgesics, including a combination of regional and intravenous analgesia. The modified thoracolumbar interfascial plane (TLIP) block is an interfascial block that targets the dorsal rami of the thoracolumbar nerve by injecting several local analgesics between the iliocostalis and longissimus dorsi muscles. The modified TLIP block is easier to perform and has a better spread of local anesthetic from classical TLIP block [3, 4]. The modified TLIP block can be an option to reduce post-spinal decompression surgery and reduce postoperative complications due to postoperative pain and opioid use [5].
In patients with cirrhosis of the liver, side effects of analgesics are common and potentially fatal [6]. Cirrhotic patients often suffer from thrombocytopenia due to increased platelet sequestration in the spleen and reduced production of thrombopoietin in the liver [7]. In this case, regional anesthesia may pose a serious risk of bleeding or hematoma. Appropriate analgesic drugs and techniques are urgently needed for pain management in patients with liver failure hepatic cirrhosis patients with thrombocytopenia.
2. CASE PRESENTATION
A 67-year-old man with right leg pain caused by L4-L5, L5-S1 lumbar canal stenosis, and L4-L5 spondylolisthesis would undergo endoscopic spinal decompression with laminotomy L4-L5 flavectomy. He had suffered liver cirrhosis for three years due to hepatocellular carcinoma, which had been treated with radiofrequency ablation. He was now on propranolol treatment 3x20 mg orally. He had a low thrombocyte count (57,000/mm3), but other coagulation factors were still within normal limits. His prothrombin time was 11,8 sec, activated partial thromboplastin time was 32,5 sec, fibrinogen level was 264 ml/dL, and D-dimer level was 4.700 ng/mL. He also suffered from acute on chronic kidney disease, with a blood creatinine level of 1.3 mg/dL and a blood urea level 46.7 mg/dL.
He was planned to have general anesthesia and a modified TLIP block. Before induction of anesthesia, his recorded blood pressure (BP) was 143/86 mmHg, heart rate was 58 bpm, peripheral oxygen saturation was 99% and the temperature was 36.5°C. After placement of routine monitors and preoxygenation, general anesthesia was induced with midazolam 1,5 mg, fentanyl 150 mcg, propofol 100 mg, and rocuronium 1mg/kg, and the patient's trachea was intubated with a 7,5 mm outer diameter endotracheal tube without any difficulty. The lungs were ventilated with a pressure control mode with tidal volume 8 ml/kg BW, respiratory rate 12/min, and PEEP 5 cmH2O with FiO2 50%. and 1% sevoflurane. He was placed in the prone position and prepared for an ultrasound-guided modified TLIP block (Fig. 1).
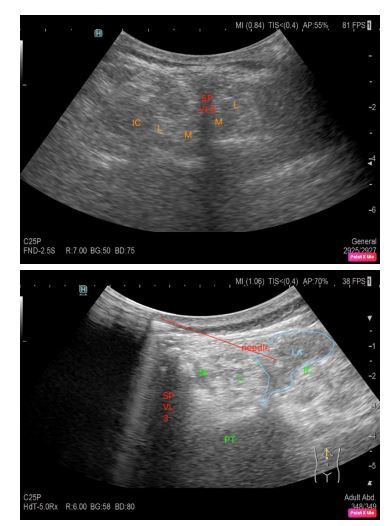
An anesthesiologist performed the modified TLIP block with a convex probe 1-6 MHz Hitachi AriettaR 750 VE, preceded by asepsis and antisepsis around the L3 vertebra. The left and right longissimus and iliocostalis muscles were identified by performing scanning on the left and right lateral sides. A 22-gauge, 100-mm block needle was inserted in a medial-to-lateral direction into the interfacial plane. Once the needle tip had been placed within the interfacial plane and after aspiration to exclude intravascular needle placement, 2 mL of saline was injected to confirm the actual injection site. Bupivacaine 0.25% 20 ml, with a total dose of 40 ml, was administered between the longissimus and iliocostalis muscles on both sides. The surgery was uneventful, and there was no complication during the surgery. Intraoperative hemodynamics was relatively stable with a systolic blood pressure range of 90-110 mmHg and a pulse rate of 60-70x/minute, SpO2 99%. Intravenous fentanyl 50 mcg was added while the surgeon made the first incision. No further addition of opioids was required intraoperatively until the surgery was completed. The patient was administered 0.01 mg/kg atropine iv and 0.02 mg/kg neostigmine and extubated at the end of the surgery. The patient’s visual analog score (VAS) at the PACU was 2; therefore, no analgesic was administered. The patient was discharged from the PACU to the ward after a modified Aldrete score of 9.
For postoperative analgesia, patient was given intravenous paracetamol 1 gram/ 8 hour. PCA was used with 1 mg morphine, 5 min lock-out interval, and a maximal dose of 4 mg/ hour. During the first 24 hours of postoperative monitoring, there was no episode of moderate or severe pain. The patient’s VAS was 1-2 in the first 24h postoperative and no additional opioid was required. No bleeding complications or hematomas were found at the TLIP block site. Likewise, no neurologic complications were found in the first five postoperative days, including spinal hematoma or nerve root compression.
3. DISCUSSION
In this presented case, the modified technique TLIP block could be performed quickly and easily by an anesthesiologist. There were also no complications of modified TLIP block in the form of nerve damage, bleeding and hematoma found perioperatively. The TLIP block can provide adequate analgesia during and after surgery, marked by stable intraoperative hemodynamic and low postoperative pain VAS without any additional opioids needed.
The liver is the main site of the biotransformation of most opioids. The administration of opioids in cirrhotic patients can increase the risk of hepatic encephalopathy. By reducing opioid requirement while providing a good analgesic effect up to 24 hours postoperatively, a modified TLIP block may be beneficial for patients with portal hypertension and encephalopathy who will undergo spinal surgery [6].
Paracetamol is often avoided in patients with liver cirrhosis, mainly because of concerns about the hepatotoxic effects of an overdose of this drug. A literature review stated that paracetamol up to 4 grams/day was well tolerated by patients with cirrhosis. The American Liver Foundation recommends taking paracetamol not more than 3 grams/day for any duration of time. In these patients, the administration of paracetamol is still within the recommended limits.
There are currently minimum data on the safety of modified TLIP interfacial blocks in patients with thrombocytopenia. The TLIP block was performed in these patients with the consideration of providing a benefit that previously had been described above. In addition, the selection of this block was also based on the consideration of normal coagulation factors level and coagulation test results, although the patient had suffered from thrombocytopenia.
There is no evidence to suggest that TLIP blocks can be performed safely in patients with coagulopathy or on anticoagulants. Some practitioners consider plana blocks, such as TLIP blocks, to be quite safe when performed in patients with coagulation disorders. Galacho found that the Erector Spinae Block (ESP) interfacial block was safe enough to perform in 5 patients with coagulation disorders (international normalized ratio (INR) more than 1.5 times normal, platelet count less or equal to 80000/μl, or currently on anticoagulant therapy) [8] Similar results were obtained by Navaro et al. in patients undergoing thoracoscopic procedures [9].
Cases of hematoma after interfacial block have been reported. Shirozu et al. reported the occurrence of hematoma following transversus abdominis plane block in a patient with HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count) [10] The Regional Anesthesia and Acute Pain Section of the Canadian Anesthesiologists Society (CAS) classifies TLIP and ESP blocks as blocks with low risk for bleeding complications or severe hematoma [11]. The American Society of Regional Anesthesia and Pain Medicine advises caution in performing deep regional anesthetic procedures in patients with coagulation disorders or on anticoagulant therapy [12].
This case reports the modified TLIP block technique was an effective and safe analgesic technique for patients with liver cirrhosis and thrombocytopenia. However, randomized controlled trials are needed to determine the safety limits of the modified TLIP block technique in patients with coagulation disorders or taking anticoagulants. This case nevertheless demonstrates the importance of appropriate choice of regional anesthesia technique and postoperative analgesia tailored to the patient’s condition and surgical technique.
CONCLUSION
Modified TLIP block can be an effective and safe analgesic technique performed in patients with hepatic cirrhosis with thrombocytopenia. However, further research is needed to determine the safety limits of modified TLIP block in patients with coagulation disorder or anticoagulant use.
LIST OF ABBREVIATIONS
| TLIP | = Thoracolumbar Interfascial Plane |
| BP | = Blood Pressure |
| VAS | = Visual Analog Score |
| ESP | = Erector Spinae Block |
| INR | = International Normalized Ratio |
| CAS | = Canadian Anesthesiologists Society |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval was obtained from The Health Research Ethics Committee at the University of Indonesia and Dr. Cipto Mangunkusumo General Hospital (KET-1093/UN.2F1/ETIK/ PPM.00.02/2020).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans were used by the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/ 3931).
CONSENT FOR PUBLICATION
Written informed consent for publication of their details was obtained from the patient.
STANDARDS OF REPORTING
CARE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the manuscript.
FUNDING
None.
CONFLICT OF INTEREST
The authors declared no conflict of interest
ACKNOWLEDGEMENTS
Declared none.

