All published articles of this journal are available on ScienceDirect.

Analgesic Efficacy of Unilateral Quadratus Lumborum Block (Lateral Approach) compared with Erector Spinae Plane Block in Patients Undergoing Unilateral Lower Abdominal Surgery (Prospective Randomized Comparative Double-blinded Clinical Trial)
Authors Info & Affiliations
Abstract
Introduction
Ultrasound-guided truncal blocks such as quadratus lumborum (QLB) and erector spinae plane block (ESPB) are increasingly used for opioid-sparing analgesia. We aimed to evaluate the postoperative analgesic outcome of ultrasound-guided unilateral QLB (lateral approach) and ESPB for use in adult patients undergoing unilateral lower abdominal surgery.
Methods
In this randomized comparative clinical trial, 48 adult patients scheduled for unilateral lower abdominal surgery were randomized to receive QLB (n = 24) and ESPB (n = 24) following induction of general anesthesia. The primary outcome was total morphine consumption in the first 24 postoperative hours.
Results
There was no statistical difference for total morphine consumption between the QLB and ESPB groups (5.26 ± 2.17 mg vs. 5.88 ± 2.51 mg; p = 0.376). The median time to first rescue analgesia was greater in the QLB (2 hours [0–18]) vs. the ESPB group (1 hour [0–21]; p = 0.251). Pain scores were not different between groups at 2, 4, 8, 12, and 24 hours post-op (median Visual Analogue Scale (VAS) at 24h: 3 [3–5] QLB, 3 [2–3] ESPB; p = 0.08). There were no differences between groups with respect to hemodynamic parameters, adverse events (nausea and vomiting: 4 in the QLB group, 6 in the ESPB group; p > 0.05) or block performance times (median time: 10min for both).
Discussion
We consider the clinical role of QLB and ESPB as an effective component of multimodal analgesia in unilateral lower abdominal surgeries. They have a similar safety profile considering the technique and the opioid sparing effects, similar performance characteristics and complication rates, which together suggest both blocks are safe and well-tolerated anesthetic procedures that can be daily practices.
Conclusion
Both QLB and ESPB provide significant, safe, and comparable postoperative analgesia for patients undergoing unilateral lower abdomen surgery. QLB may provide a slight time benefit to analgesia onset.
Clinical Trial Registration No
This study was prospectively registered on ClinicalTrials.gov (NCT05524038; principal investigator: Rana Ahmed Abdelghaffar), registration date: 1/9/ 2022.
1. INTRODUCTION
Postoperative pain is a significant problem following abdominal surgery, even after relatively minor surgery [1-3]. Most pain postoperatively arises from the abdominal wall and, unless managed effectively, can cause chronic pain in up to 12% of patients and disrupt everyday function and quality of life [4]. In recent years, regional anesthesia techniques using ultrasound have revolutionized pain control through direct visualization of the nerve anatomy and, consequently, improved block success and precision [5]. Among the regional anesthesia techniques, abdominal wall blocks have become the more favored choices for postoperative wound pain relief, the reduction of surgical stress, accelerated recovery, and improved outcomes [6, 7].
The quadratus lumborum block (QLB) has gained recognition as an effective method for managing somatic pain following both upper and lower abdominal procedures [8-10]. First introduced by Blanco, the technique has since been adopted across a wide range of patient populations, including children, pregnant women, and adults [11]. In practice, QLB has proven useful for managing pain after a variety of operations, including laparoscopic, orthopedic, and abdominal surgeries. Its effect typically lasts up to 48 hours, offering extended relief through a single injection. To maintain or boost this duration, some clinicians prefer a continuous infusion through a catheter, while others combine the block with additives such as magnesium or dexamethasone [8]. There are several variations of the technique, including the lateral and transmuscular (QLB-T) approaches; the latter was described by Dam et al. In this study, the lateral approach was chosen for its ease of performance and consistent effectiveness, particularly in lower abdominal surgical cases [12].
Forero first presented the Erector Spinae Plane Block (ESPB), another interesting interfascial block first designed to control thoracic neuropathic pain [13]. Considered safer than conventional paravertebral blocks, ESPB is easy to perform and targets bony landmarks rather than delicate paravertebral spaces [14]. By spreading local anesthetic into the paravertebral and possibly epidural spaces, ESPB offers a major advantage in blocking both somatic and visceral pain [15-18]. Originally used for thoracic pain, ESPB has lately been used in upper abdominal, breast, and even pediatric abdominal operations [16, 19-21]. As they offer efficient opioid-sparing analgesia [4, 22], Ultrasonic-guided truncal blocks like QLB and ESPB have become rather common in abdominal operations. Particularly, QLB-II (and ESPB have shown advantages in both acute and chronic pain contexts [23, 24]. Still, there is little data directly comparing their effectiveness, particularly in unilateral lower abdominal surgeries.
In our study, we hypothesized that a unilateral Quadratus Lumborum Block (lateral approach) can provide an effective analgesia comparable with the Erector Spinae Plane Block (ESPB).
The objective of this randomized comparative clinical study is to assess, in adult patients undergoing unilateral lower abdominal surgery, the analgesic efficacy of ultrasound-guided unilateral Quadratus Lumborum Block (lateral approach) against Erector Spinae Plane Block (ESPB). The degree of pain relief, block accuracy, hemodynamic stability, and complication rates are the main subjects of comparison.
2. METHODS
This randomized clinical trial was conducted at Fayoum University Hospitals, located in Fayoum, Egypt, and included a total of 48 adult patients scheduled for unilateral lower abdominal surgical procedures. This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the affiliated institution. Prior to initiating the study, approval was granted by the Ethics Committee of the Faculty of Medicine, Fayoum University, Egypt (D237). All participants gave informed written consent before enrollment.
2.1. Eligibility Criteria
Participants were men or women between 18 and 60 years of age, classified as American Society of Anesthesiologists (ASA) physical status I or II. All were scheduled to undergo elective lower abdominal procedures such as inguinal hernia repair, hydrocele excision, or orchiopexy under general anesthesia.
2.2. Exclusion Criteria
Patients were excluded if they refused to participate or had any of the following: coagulation disorders, skin infection or lesions at the intended injection site, allergy to local anesthetics or opioids, known neurological or psychiatric illness, opioid use within the 48 hours prior to surgery, a body mass index (BMI) greater than 35 kg/m2, or an inability to clearly visualize anatomical landmarks using ultrasound.
2.3 Blinding and Randomization
Computer programs generated random number sequences and assigned participants to one of two study groups. Each assignment was placed in a sealed, non-transparent envelope that was opened just at the intervention
2.3.1. Preoperative Assessment and Anesthetic Induction
A comprehensive medical and surgical evaluation was performed on each participant. This included complete blood counts, standard laboratory tests, renal and hepatic function panels, coagulation parameters such as prothrombin concentration, partial thromboplastin time, and international normalized ratio, and a thorough clinical evaluation. An electrocardiogram was performed for patients older than forty years or those with clinical indications. Additional diagnostic investigations were ordered based on individual comorbid conditions. Prior to surgery, each patient was thoroughly instructed on how to report postoperative pain using the visual analogue scale, where a score of zero indicated no pain and a score of ten reflected the most severe pain imaginable.
Standard monitoring was started as soon as the patient entered the operating room, following the guidelines set forth by the American Society of Anesthesiologists. This included capnography monitoring, continuous electrocardiographic tracing, pulse oximetry, and noninvasive blood pressure measurement. Each patient's heart rate, mean arterial pressure, systolic and diastolic blood pressure, and peripheral oxygen saturation were recorded. Intravenous cannulation (IV) and intravenous fluid were started. Intravenous Midazolam 0.03-0.05 (mg/kg) was administered to all patients as a premedication. Then, general anesthesia was given for both groups, with intravenous injection of fentanyl 1-2 micrograms per kilogram (μg/kg), propofol (1.5 - 2 mg/kg).
To facilitate endotracheal intubation, 0.5 milligrams(mg) of atracurium per kilogram(kg) was administered. Following intubation, all patients were mechanically ventilated using the controlled mechanical ventilation mode. The tidal volume was set between six and eight milliliters per kilogram(ml/kg), and a gas mixture of oxygen and air in equal proportions was used to maintain end-tidal carbon dioxide between thirty and forty millimeters of mercury. Isoflurane at concentrations between one and two percent was used to maintain general anesthesia. Atracurium doses of 0.1 milligrams per kilogram were administered at intervals of 20 to 30 minutes. An additional dose of fentanyl at 0.5 micrograms per kilogram was given if the mean arterial pressure or heart rate increased by more than 20% from the preoperative baseline values. Among the hemodynamic parameters that were continuously monitored were heart rate, mean arterial pressure, and peripheral oxygen saturation. These measurements were obtained prior to the procedure, during the procedure up to 135 minutes at 15-minute intervals, and at 0, 2, 4, 8, 12, and 24 hours following the procedure.
The attending anesthesiologist used the approved regional anesthesia technique after the surgery was finished and before the patient emerged from anesthesia. This affected either the erector spinae plane block or the quadratus lumborum block. With a high-frequency linear ultrasound probe, the Active Array L12-4 probe, which operates at eight to thirteen megahertz, connected to a Philips Clear Vue 350 ultrasound system, both procedures were carried out in a completely aseptic environment. To ensure hygienic conditions, a sterile cover was utilized. The injections were administered with a 22-gauge, 50-millimeter echogenic needle (Stimuplex D; B. Braun, Germany). Single-sided lateral approach QLB was administered to patients in the quadratus lumborum group. A one-sided ESPB was performed on patients in the erector spinae group.
2.3.2. Regional Block Techniques and Immediate Postoperative Care
Patients in the quadratus lumborum group were positioned laterally during the procedure. Just above the iliac crest, a high-frequency linear ultrasound probe was positioned. The transversus abdominis muscle was followed posteriorly until its aponeurotic termination was visible, and the three different layers of the abdominal wall musculature were identified. After that, the probe was angled slightly caudally into the pelvic area to make the tapered end of the aponeurosis more visible. In most cases, the quadratus lumborum muscle was located medially to the transversus abdominis aponeurosis. The needle was advanced from a supero-anterior to a postero-inferior direction using an in-plane technique, aiming for the anterolateral surface of the quadratus lumborum at its interface with the transversalis fascia. Twenty milliliters of 0.5 percent bupivacaine and four milligrams of dexamethasone were injected after ultrasound guidance verified that the local anesthetic had spread beneath the aponeurosis.
In the erector spinae group, patients were also placed in the lateral decubitus position. Following antiseptic preparation of the skin using ten percent povidone iodine, the ultrasound probe was applied approximately one to two centimeters lateral to the midline at the lumbar spine. Tracing upward from the sacrum, the first lumbar vertebral level was located. Next, the erector spinae muscle and transverse process were seen. The in-plane technique was used to insert a needle deep into the erector spinae muscle in a craniocaudal direction. The correct position of the needle tip was verified by injecting a small test dose of local anesthetic between 0.5 and 1 milliliter. Once the needle placement was confirmed, a total volume of twenty milliliters of 0.5 percent bupivacaine and four milligrams of dexamethasone was delivered at the site.
Anesthesia was stopped after the procedure was completed. Neostigmine, at a dose of 0.04 to 0.08 milligrams per kilogram, and atropine, at a dose of 0.02 milligrams per kilogram, were used to reverse residual neuromuscular blockade. After regaining full consciousness and meeting the extubation requirements, each patient was carefully extubated and transported to the post-anesthesia care unit for further monitoring. Each participant received a regular analgesic regimen during the recovery period.
As part of the usual pain management protocol, one gram of intravenous paracetamol was administered to each participant every six hours. Three milligrams of morphine were injected intravenously as a rescue dose if a patient reported a visual analogue scale (VAS) score higher than three. If the pain continued after half an hour, this dosage could be repeated until the VAS score dropped below four.
2.3.3. Pain Score Assessment
The VAS was used to measure pain intensity at predetermined intervals after surgery by a second anesthesiologist who was blinded to group allocation. These included four, eight, twelve, and twenty-four hours following the procedure's completion, as well as the immediate postoperative period (zero hours).
Patients were closely monitored in the post-anesthesia care unit for potential adverse effects. Hypotension was defined as a reduction in mean arterial pressure by twenty percent or more from baseline values and was managed with fluid resuscitation and intravenous ephedrine. Bradycardia, which is defined by at least a twenty percent drop in heart rate from baseline, was treated with intravenous atropine, a dose of 0.02 mg/kg. The evaluation of respiratory depression was identified with an oxygen saturation of less than ninety-five percent, which was treated with supplemental oxygen therapy. Postoperative nausea and vomiting were recorded and treated as necessary.
2.4. Study Outcomes
2.4.1. Primary Outcome
The main objective of this study was to compare the total amount of opioid analgesics, specifically morphine, administered within the first twenty-four hours after surgery between the two intervention groups.
2.4.2. Secondary Outcomes
Hemodynamic Monitoring: mean arterial pressure, heart rate, and O2 saturation were recorded at baseline, at 15-minute intervals during the procedure (15, 30, 45, 60, 75, 90, 105, 120, and 135 minutes), and at predetermined times after surgery (0, 2, 4, 8, 12, and 24 hours).
Time to the first use of analgesic(morphine) [time frame: 24 hours], number of doses for each patient, and total amount needed.
Postoperative pain measurements using the visual analogue scale at the following time points: immediately after surgery and then at 2, 4, 8, 12, and 24 hours.
Patient Satisfaction with the overall management of postoperative pain was scored 24 hours after surgery using a four-point scale (0 = poor; 1 = fair; 2 = good; 3 = excellent).
Block-related complications: bowel injury, hematoma, inadvertent intravascular injection, pruritus, nausea, vomiting, hemodynamic instability, systemic toxicity from local anesthetic, and infection at the injection site.
Technical feasibility was assessed via the time to perform the block and the number of attempts with the needle.
2.5. Sample Size Calculations
Sample size calculation was performed using G*power version 3.1.9.2 (Kiel University, Kiel, Germany) software [25]. In a recent similar study performed by Yousef NK, we calculated the dose of morphine in the first 24 hours, which is our primary outcome [26]. This study showed that the mean opioid consumption at 24 hours was 14.46 ± 3.4 for the TAPB group and 10.06 ± 3.8 for the QLB group. The sample size was calculated at a power 95% and a significance level of 5%, and an allocation ratio between the two groups of 1:1. This analysis showed that 19 patients will be required for each group to obtain a significant statistical value. 23 patients for each group (with a total of 46 patients) were included in the study for the possibility of patient dropouts.
2.6. Statistical Analysis
All data analyses were conducted with version 27 of the Statistical Package for the Social Sciences (SPSS), developed by IBM Corporation, Armonk, New York, United States. The distribution of continuous variables was evaluated with the Shapiro-Wilk test and visually through examining histograms. Continuous variables with a normal distribution were summarized as mean with standard deviation; with comparisons between groups conducted using an independent samples t-test. Categorical variables were summarized as frequency and percentage. Categorical group comparisons were conducted using either the Chi-square test or Fisher's exact test when expected frequencies were low. Statistical significance is indicated with a p-value <0.05 (2-tailed).
3. RESULTS
In this Randomized controlled trial, 60 patients scheduled for unilateral lower abdominal surgical procedures were assessed for eligibility. While 12 patients were excluded, 48 patients were randomized into two groups receiving either an ultrasound-guided ESPB or Unilateral Quadratus Lumborum Block with an allocation ratio of 1:1. All patients were followed up and analyzed statistically (Fig. 1).
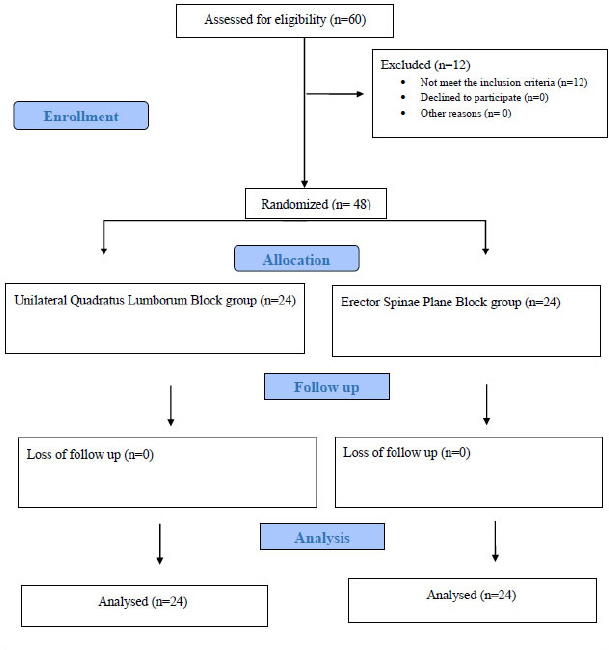
CONSORT flowchart of the study population.
3.1. Primary Outcome
3.1.1. Postoperative Opioid Consumption
Table 1 indicates there was no statistically significant difference between the two groups for either the number of morphine doses or the amount of morphine (mg). In terms of morphine doses, 37.5% of patients in group I required only one dose of morphine, while 20.8% of patients in group II. Two doses of morphine were used by 37.5% of group I and 45.8% of group II. Three doses were utilized by 16.7% in group I and 25% in group II. Mean amount of the first dose of morphine was 2.96mg (SD 0.64) in group I, compared to 2.83mg (SD 0.92) in group II. For the second dose, the mean was 2.71 milligrams (SD 0.61) in Group I and 2.42 milligrams (SD 0.61) in Group II. For patients who needed a third dose, the mean was 2.25 milligrams (SD 0.50) in Group I and 2.75 milligrams (SD 0.89) in Group II. The mean for a fourth dose was only administered to a small number of patients and was an average of 3.00 milligrams (SD 0.00) in Group I and 2.50 milligrams (SD 0.70) in Group II. In summary, the mean total morphine requirements during the first 24 hours after surgery were 5.26 milligrams (SD 2.17) in Group I and 5.88 milligrams (SD 2.51) in Group II.
| Number and Amount of Doses of Morphine Among Studied Groups | ||||
|---|---|---|---|---|
| Category | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| Number of Doses | MC = 3.08 | 0.545 | ||
| 0 | 1 (4.2%) | 0 (0.0%) | ||
| 1 | 9 (37.5%) | 5 (20.8%) | ||
| 2 | 9 (37.5%) | 11 (45.8%) | ||
| 3 | 4 (16.7%) | 6 (25.0%) | ||
| 4 | 1 (4.2%) | 2 (8.3%) | ||
| Amount of 1st dose (mg) | 3 ± 0.6 | 2.9 ± 1 | t = 0.532 | 0.597 |
| Amount of 2nd dose (mg) | 2.7 ± 0.6 | 2.4 ± 0.6 | t = 1.37 | 0.181 |
| Amount of 3rd dose (mg) | 2.3 ± 0.5 | 2.8 ± 0.9 | t = 1.03 | 0.326 |
| Amount of 4th dose (mg) | 3.0 ± 0.0 | 2.5 ± 0.7 | t = 0.577 | 0.667 |
| Total morphine 24h (mg) | 5.3 ± 2.2 | 5.9 ± 2.6 | t = 0.895 | 0.376 |
| Analgesic Characteristics Among Studied Groups | ||||
| Characteristic | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| Time to 1st analgesic (hours) | 2 (0–18) | 1 (0–21) | z = 1.14 | 0.251 |
| Time between 1st & 2nd dose (hours) | 5 (2.5–18) | 6 (1.5–15) | z = 0.438 | 0.661 |
| Time between 2nd & 3rd dose (hours) | 9 (8–18) | 11.5 (8–15) | z = 0.295 | 0.769 |
| Time between 3rd & 4th dose (hours) | 12 (12–12) | 5.5 (5–6) | z = 1.23 | 0.221 |
| General Satisfaction Among Studied Groups | ||||
| Satisfaction Level | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| 1 | 7 (29.2%) | 9 (37.5%) | X2 = 0.752 | 0.686 |
| 2 | 13 (54.2%) | 10 (41.7%) | ||
| 3 | 4 (16.7%) | 5 (20.8%) | ||
Note: Parameters described as median (range), Z: Mann Whitney U test.
3.2. Secondary Outcomes
3.2.1. Baseline Characteristics
Demographic and clinical characteristics of each group are shown in Table 2. There were no statistically significant differences between the groups for age, sex distribution, body mass index, or ASA physical status classification. The mean age in the quadratus lumborum group (Group I) was 34.92 years (SD 11.96), and the erector spinae group (Group II) was 34.17 years (SD 13.52). The proportion of males from each group was 70.8 percent. The mean (SD) for body mass index was 26.62 kg/m2 (SD 3.93) in Group I and 26.40 kg/m2 (SD 3.09) in Group II. Regarding ASA status, 91.7 percent of patients in Group I were ASA I and 8.3 percent were ASA II; while 75 percent in Group II were ASA I and 25 percent were ASA II. There was no statistically significant difference in ASA classification between groups (p = 0.12).
| Demographic Characteristics Among Studied Groups | ||||
|---|---|---|---|---|
| Variable | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| Age (years) | 34.9 ± 12 | 34.1 ± 13.6 | t = 0.204 | 0.84 |
| Sex | χ2 = 0.0 | 1 | ||
| - Male | 17 (70.8%) | 17 (70.8%) | ||
| - Female | 7 (29.2%) | 7 (29.2%) | ||
| BMI (kg/m2) | 26.6 ± 4 | 26.4 ± 3.1 | t = 0.216 | 0.83 |
| ASA Score | χ2 = 2.4 | 0.12 | ||
| - ASA I | 22 (91.7%) | 18 (75.0%) | ||
| - ASA II | 2 (8.3%) | 6 (25.0%) | ||
| Surgery Characteristics Among Studied Groups | ||||
| Variable | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| Type of Surgery | χ2 = 0.0 | 1 | ||
| - Inguinal | 9 (37.5%) | 9 (37.5%) | ||
| - Appendectomy | 15 (62.5%) | 15 (62.5%) | ||
| Duration of Surgery (min) | 65.6 ± 33.3 | 53.1 ± 16.5 | t = 1.65 | 0.107 |
Note: t: Student t test, X2:Chi –Square test, *statistically significant.
3.2.2. Hemodynamic Parameters
As presented in Table 3, there were no significant differences in mean arterial pressure. The mean arterial pressure in group I is presented at 84.88 mmHg (SD 16.48) preoperatively, as compared to 76.00 mmHg (SD 0.83) at 24 hours postoperatively. In group II, the average samples were 93.38 mmHg (SD 15.37) preoperatively and 77.08 mmHg (SD 3.86) at 24 hours postoperatively.
| Time Point | Group I (N=24) | Group II (N=24) | t-value | p-value |
|---|---|---|---|---|
| Mean Arterial Pressure (MAP) Changes | ||||
| Post-op 0 h | 85.1±16.3 | 90.2±10.2 | 1.29 | 0.202 |
| Post-op 2 h | 77.6±7.8 | 80.3±4.9 | 1.48 | 0.145 |
| Post-op 4 h | 83.5±2 | 83.5±1.3 | 0.087 | 0.931 |
| Post-op 8 h | 81.5±0.5 | 81.6±1.8 | 0.321 | 0.75 |
| Post-op 12 h | 79.0±0.834 | 79.88±2.19 | 1.83 | 0.074 |
| Post-op 24 h | 76.0±0.834 | 77.08±3.86 | 1.35 | 0.185 |
| O2 Saturation Changes | ||||
| Post-op 0 h | 97.92±2.04 | 98.83±1.37 | 1.83 | 0.074 |
| Post-op 2 h | 97.0±0.834 | 97.0±0.834 | 0 | 1 |
| Post-op 4 h | 97.67±1.31 | 98.12±1.12 | 1.31 | 0.198 |
| Post-op 8 h | 97.54±1.44 | 98.25±0.794 | 2.11 | 0.051 |
| Post-op 12 h | 97.54±1.79 | 98.08±1.41 | 1.16 | 0.251 |
| Post-op 24 h | 97.58±1.53 | 98.04±1.23 | 1.14 | 0.259 |
| Heart Rate Changes | ||||
| Post-op 0h | 79.5 ± 10.5 | 87.7 ± 18.4 | t = 1.90 | 0.063 |
| Post-op 2 h | 78.3 ± 8.9 | 81.3 ± 10.4 | t = 1.08 | 0.288 |
| Post-op 4 h | 78.6 ± 8.4 | 82.3 ± 10.3 | t = 1.33 | 0.189 |
| Post-op 8 h | 78.5 ± 8.5 | 83.1 ± 10.5 | t = 1.67 | 0.102 |
| Post-op 12 h | 78.4 ± 8.4 | 82.0 ± 8.8 | t = 1.46 | 0.152 |
| Post-op 24 h | 78.4 ± 6.3 | 82± 7.7 | t = 1.67 | 0.265 |
Note: t: Student t test *statistically significant.
Table 3 shows that there was no statistically significant difference in peripheral oxygen saturation between the groups at any time point. In Group I (in which a quadratus lumborum block was performed), mean oxygen saturation prior to surgery was 97.79% (SD 1.89) and decreased slightly to 97.58% (SD 1.53) at the 24-hour postoperative evaluation. In Group II (where an erector spinae plane block was performed), mean oxygen saturation prior to surgery was 98.54% (SD 2.02), which decreased only slightly to 98.04% (SD 1.23) during the last recorded 24-hour postoperative evaluation.
There was no statistically significant difference between the groups with regard to mean pre-operative, intraoperative, and post-operative heart rate (Fig. 2). For group I(QLB); mean preoperative heart rate was 79.38±12.92, which changed to 78.35±6.29 at the last follow-up post-operative assessment at 24 hours. For group II (ESPB); mean preoperative heart rate was 84.71±19.78, which became 81.98±7.71 at the last follow-up post-operative assessment at 24 hours, as shown in Table 3.
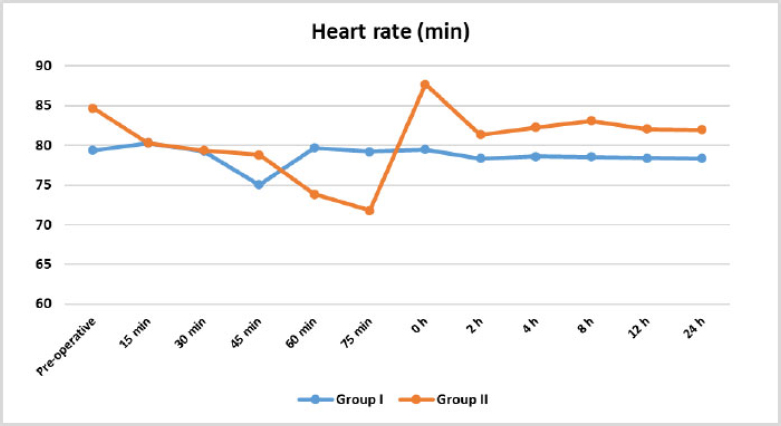
Heart rate changes during follow up between studied groups.
3.2.3. Time to Analgesic Use and Intervals among Doses
Table 1 shows no statistically significant differences between the two groups in terms of the timing of analgesic administration. The median time to the first request for analgesia was 2 hours in Group I (quadratus lumborum block), with a range of 0 to 18 hours. In comparison, Group II (erector spinae block) had a median of 1 hour, ranging from 0 to 21 hours. The median time interval between the first and second morphine doses was 5 hours in Group I and 6 hours in Group II. Subsequent intervals between the second and third doses, as well as between the third and fourth doses, also showed no statistically significant variation between the groups.
3.3. Postoperative Pain Scores
Pain intensity, assessed using the visual analogue scale (VAS), did not differ significantly between the two groups throughout the 24-hour postoperative period, as shown in Table 4. At zero hours postoperatively, the value of the VAS score (median) for both groups was 3 (range 0 to 7). At 24-hour postoperative time, the score in Group I was 3 (range 3 to 5) and in Group II was 3 (range 2 to 3).
3.4. Patient Satisfaction
No significant differences were observed between the groups with respect to overall satisfaction with postoperative pain control. In Group I, 54.2 percent of patients rated their satisfaction as “good” (score 2), 29.2 percent as “fair” (score 1), and 16.7 percent as “excellent” (score 3). In Group II, 41.7 percent reported “good” satisfaction, 37.5 percent reported “fair,” and 20.8 percent rated their experience as “excellent.” These findings are presented in Table 1.
3.5. Surgical Variables
There were no significant differences between the groups in terms of type of surgical procedure or surgery duration, as shown in Table 2.
3.6. Technical Performance of Regional Blocks
As shown in Table 4, there were no statistical differences between groups for ease of performing the regional blocks using time for the procedure and the number of attempts. The median time for the regional procedure within Group I (quadratus lumborum block) was 10 minutes, and the range was 5-10 minutes. The median for the regional procedure in Group II (erector spinae block) was also 10 minutes.
| VAS Score Distribution Among Studied Groups | ||||
|---|---|---|---|---|
| Time Point | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| 0 h | 3 (0–7) | 3 (0–7) | z = 1.42 | 0.154 |
| 2 h | 3 (0–5) | 3 (2–5) | z = 0.899 | 0.369 |
| 4 h | 3 (0–7) | 3 (2–5) | z = 1.31 | 0.191 |
| 8 h | 3 (0–5) | 3 (2–7) | z = 0.084 | 0.933 |
| 12 h | 3 (2–7) | 3 (2–5) | z = 0.394 | 0.693 |
| 24 h | 3 (3–5) | 3 (2–3) | z = 1.77 | 0.08 |
| Time Required and Number of Attempts Distribution | ||||
| Variable | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| Time required (min) | 10 (5–20) | 10 (5–25) | z = 0.402 | 0.688 |
| Number of attempts | 2 (1–5) | 2 (1–5) | z = 0.215 | 0.83 |
| Side Effects Distribution Among Studied Groups | ||||
| Side Effect | Group I (N=24) | Group II (N=24) | Test Statistic | p-value |
| Nausea | 2 (8.3%) | 3 (12.5%) | FET = 0.223 | 1 |
| Vomiting | 2 (8.3%) | 3 (12.5%) | FET = 0.223 | 1 |
| Intravascular injection | 0 | 0 | — | — |
| Hematoma formation | 0 | 0 | — | — |
| Bowel injury | 0 | 0 | — | — |
| Pruritis | 0 | 0 | — | — |
| Hemodynamic instability | 0 | 0 | — | — |
| Signs of local toxicity | 0 | 0 | — | — |
| Infection at injection site | 0 | 0 | — | — |
Note: Parameters described as median (range), Z: Mann Whitney U test.
3.7. Adverse Events
The rate of postoperative complications was low and similar between groups, with no statistical differences. In Group I 2 patients had postoperative nausea, and 2 patients reported conclusive vomiting. In Group II, 3 patients were identified with nausea, and 3 patients had vomiting. No other complications were documented regarding hematoma, pruritus, hemodynamic instability, local anesthetic systemic toxicity, and infection at the injection site as shown in Table 4.
4. DISCUSSION
The current prospective randomized comparative double-blinded parallel group clinical trial study assessed the analgesic efficacy of ultrasound-guided quadratus lumborum block (QLB) by the lateral approach compared to erector spinae plane block (ESPB) in adult patients undergoing unilateral lower abdominal surgery. The total morphine consumption was slightly higher in the ESPB group, this difference was not statistically significant. As regards oxygen saturation, there were minor variations, with the ESPB group showing slightly higher oxygen saturations at certain time points; still, these values were within the range of normal physiology. Most other outcomes found no statistically significant differences between the groups. These outcomes included baseline characteristics (age, sex, BMI, ASA score), surgical parameters (procedure type, procedure duration), and hemodynamic measures (heart rate and mean arterial pressure). There were also no statistically significant differences between groups for time of first analgesic dose, the number or quantity of morphine doses, pain scores at all time points, patient satisfaction, adverse events, or technical performance of the block.
In accordance with our data, AbdEllatif and Abdelnaby [16] reported no significant differences in heart rate (HR) or mean arterial pressure (MAP) between the QLB and ESPB groups in patients undergoing open nephrectomy. Similarly, Zanfini et al. [17] demonstrated no significant hemodynamic differences between the two groups. Contrarily, in a study of patients undergoing laparoscopic hysterectomy, Baran [18] determined significantly greater intraoperative MAP and HR in the QLB group compared with the ESPB and Control groups, possibly due to differing sample size or surgical procedure. In terms of opioid consumption, we identified no significant difference between groups in the number of morphine doses or the total 24-hour morphine requirement. In the same line, Elkhodary et al. [27] conducted a randomized, double blind trial study on 75 cases that underwent open nephrectomy surgeries, stating that the total dose of morphine during the first 24 hours was insignificantly different between QLB and ESPB groups. These results are consistent with AbdEllatif and Abdelnaby [16] and Aksu et al. [19], who both reported similar opioid needs in QLB and ESPB groups. In contrast, Fakhry et al. [28] and Hetta et al. [29] found significantly lower opioid use in the ESPB group. The difference may be due to the possibility of bilateral blocks, local anesthetic concentration, or our regimen of adjuvants, such as dexamethasone, in our study protocol. Time to first rescue analgesia was comparable between the groups in our study, consistent with research from Abd Ellatif and Abdelnaby [16] and Aksu et al. [19]. However, Fakhry et al. [28] and Hetta et al. [29] observed a significantly prolonged duration of analgesia with ESPB. Differences in block technique or type of surgical procedure and associated discomfort patterns may help explain the discrepancy. Pain intensity, measured by VAS, showed no significant difference between groups in our study across all time points. Similar findings were reported by Elkhodary et al. [27] Aksu et al. [19], Hetta et al. [29], and Fakhry et al. [28], although the latter two noted significantly lower VAS scores in the ESPB group at selected time intervals. Zhang et al. [21] also demonstrated superior analgesia with ESPB, but this may further differ by sample size and surgical variability. We did not observe differences in procedural time or number of attempts between groups that supported the relative technical feasibility of both blocks. Adverse events like nausea and vomiting were infrequent and comparable between groups, as seen in Fakhry et al. [28], Zhang et al. [21], and Hetta et al. [29]. Lastly, patient satisfaction was similar across groups as Aksu et al. [19] stated. However, Fakhry et al. [28] did report significantly higher rates of satisfaction with the ESPB, potentially suggesting differences in patient expectation or analgesic response between groups.
The results of this study lend support for the clinical role of QLB and ESPB as effective components of multimodal analgesia in unilateral lower abdominal surgeries. Based on the similar opioid sparing effects together with the similar safety profiles of both QLB and ESPB, either block could be used equally well based on the technical ability of the provider and the logistical protocols of the institution. Furthermore, there were very similar performance characteristics and complication rates, which together suggest both blocks are safe and well-tolerated anesthetic procedures that can be daily practices.
Future research should move toward larger multicenter randomized studies to confirm the generalizability of the findings while incorporating a broader surgical population and to provide informative comparisons examining the effects of bilateral versus unilateral block application, differences in concentrations or volumes of local anesthetic, while also adding in adjuvants like clonidine or dexmedetomidine. It would also be informative to consider their effects when examining specific surgical subtypes or assessing their role in certain high-risk patients, like the obese or individuals with limited respiratory reserve.
5. LIMITATIONS
There are, however, some limitations to acknowledge. This study was conducted at a single centre; with a relatively small sample size. The lack of a third control group (no regional block) restricts our ability to quantify the absolute benefit of QLB and ESPB over systemic analgesia alone. Additionally, our findings may not be generalizable to all types of abdominal surgeries, and for patients with comorbidities not represented in our study population.
CONCLUSION
The erector spinae plane block (ESPB) and quadratus lumborum block (QLB), in contrast, have shown equivalent efficacy for postoperative analgesia following unilateral lower abdominal surgery. Neither technique had a significant advantage over the other in total opioid use, pain severity, hemodynamic stability, timing of rescue analgesia, or adverse event incidence. Future large-scale and multi-center studies from which to generalize these results and the potential for different block durations, long-term analgesic effects, and patient-reported outcomes are much needed.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: M.M.E., R.A.A., J.M.B.: Study conception and design; M.M.E., R.A.A., M.L.B.: Data collection; M.A.H., M.M.E., R.A.A., J.M.B.: Analysis and interpretation of results; M.A.H., M.M.E., R.A.A., J.M.B., M.L.B., M.M.B., F.O.B.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| QLB | = Quadratus Lumborum Block |
| ESPB | = Erector Spinae Plane Block |
| MAP | = Mean Arterial Pressure |
| SPSS | = Statistical Package for the Social Sciences |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of the Faculty of Medicine, Fayoum University, Egypt (D237).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and analyzed during the current study are available from the corresponding author (M.A.H.) upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

