All published articles of this journal are available on ScienceDirect.

Real-World Incidence and Determinants of Postoperative Nausea and Vomiting in Adult Surgical Patients: A Retrospective Cohort Study
Authors Info & Affiliations
Abstract
Introduction
Despite the availability of effective antiemetic prophylactic strategies, postoperative nausea and vomiting (PONV) is a prevalent and distressing complication following anesthesia. Understanding the real-world data on incidence of PONV, risk factors, and adherence to prophylaxis protocols is essential for enhancing perioperative care.
Objectives
The objective of this study is to determine the incidence of PONV, identify risk factors, assess the effectiveness of prophylactic antiemetic use, and assess adherence to institutional prophylactic antiemetic policy.
Method
This was a retrospective observational study on adult patients (≥18 years) undergoing inpatient surgery under general anesthesia. Data on patient demographics, Apfel risk factors, anesthesia and surgical details, antiemetic use, and PONV occurrence were retrieved from an institutional electronic database.
Results
A total of 1113 patients were analysed. The overall incidence of PONV within 24 hours after surgery was 17.9%. Patients with PONV had significantly higher ASA scores (2.6 ± 0.9 vs 2.2 ± 0.8; p<0.001), longer anesthesia duration (148.4 ± 100.6 minutes vs 127.8 ± 77.7 minutes; p=0.002), and higher Apfel scores (2.5 ± 0.7 vs 2.4 ± 0.7; p=0.032). Intraoperative antiemetic prophylaxis was associated with a significantly lower PONV incidence compared with no prophylaxis (16.9% vs 39.2%; p<0.001).
Conclusion
Patient-related factors, particularly female sex and higher Apfel score, were key determinants of PONV. Perioperative prophylaxis significantly reduced the risk of PONV. Improved adherence to institutional multimodal prophylaxis protocols may further reduce PONV and enhance postoperative recovery.
1. INTRODUCTION
Postoperative nausea and vomiting (PONV) is still one of the most common and distressing complications following anesthesia and surgery [1]. PONV remains prevalent in a substantial proportion of surgical patients despite improvement in anaesthetic techniques and the use of effective antiemetic agents; the incidence rates ranged from 30% in patients undergoing surgery to 80% in high-risk patients [2]. Patients have rated PONV as one of the most undesirable postoperative outcomes, often surpassing pain in terms of perceived discomfort and dissatisfaction [3, 4].
Moreover, PONV results in delayed recovery, prolonged post-anesthesia care unit (PACU) stay, delayed hospital discharge, higher healthcare costs, and, in severe cases, related complications, including wound dehiscence, aspiration, dehydration, and electrolyte imbalance [5-7]. Psychological consequences of PONV include anxiety, distress, embarrassment, and even fear of further surgeries. Physical and psychological complications of PONV can result in an overall negative patient experience and ultimately have implications for the facility’s overall patient satisfaction [8]. These consequences are clear indications of the necessity of effective risk stratification and preventive strategies in perioperative care. Various factors related to patients, anesthesia, and surgery have been reported to influence the risk of PONV. Female sex, non-smoking status, previous PONV or motion sickness experience, and the use of postoperative opioids are established independent factors used to predict PONV and contribute to the widely used Apfel simplified risk score. The use of volatile anaesthetics, the duration of surgery, and the type of surgical procedure are other predictors [8-10].
International consensus guidelines recommend a risk-based, multimodal implementation of PONV prophylaxis that includes consideration of one or more antiemetic agents according to the patient’s baseline risk [11]. Aligned with this, our institution is follows a standardized universal dual-antiemetic approach for most surgical patients. Although adherence to protocol-based prophylaxis reduces the incidence and severity of PONV, compliance with standard guideline recommendations in actual clinical practice is often inconsistent [11, 12]. Thus, the current study aimed to determine the incidence of PONV among adult patients undergoing inpatient surgery under general anesthesia, assess the use and effectiveness of prophylactic antiemetics, detect PONV risk factors, determine adherence to protocol-based prophylaxis, and evaluate relationships between PONV and postoperative outcomes.
2. METHODOLOGY
2.1. Study Design and Setting
This was a retrospective observational cohort study. Perioperative data retrieved from the institutional electronic clinical information system for the period from January 1, 2024, to September 30, 2025, were analysed. The study protocol was approved by the Institutional Review Board, Dubai Hospital, Dubai, UAE (IRB approval number: MBRU IRB-2025-539, dated 4 June 2025). The requirement for informed consent was waived due to the retrospective nature of the study and use of anonymized data. Patient confidentiality was strictly maintained throughout the study, and all data were de-identified prior to analysis.
2.2. Study Population
Adult patients of either sex, aged 18 years or older, who underwent inpatient surgical procedures under general anesthesia during the study period were included in the analysis. Data for this study were extracted from the institutional electronic clinical database based on predefined inclusion and exclusion criteria. Only patients with complete records for the variables of interest were included in the analysis. Hence, patients with incomplete or missing perioperative records for key outcome variables, paediatric patients, patients who underwent outpatient or day-care surgical procedures, or patients who underwent regional anesthesia alone were excluded by default.
2.3. Data Source and Data Collection
Using a predefined data abstraction form, trained investigators extracted the data from the institutional electronic clinical database. The extracted variables included demographic characteristics, smoking status, preoperative risk factors, antiemetic prophylaxis details, adherence to institutional protocol-based antiemetic prophylaxis, occurrence of PONV within 0–24 hours postoperatively, need for rescue antiemetics in the post-anesthesia care unit (PACU) and within 24 hours after PACU discharge, and length of PACU stay.
2.4. Primary Outcome
The primary outcome was the incidence of PONV occurring within 24 hours after surgery, defined as the presence of nausea and/or vomiting documented in PACU or postoperative records.
2.5. Secondary Outcomes
Secondary outcomes included the effectiveness of prophylactic antiemetic regimens, requirement for rescue antiemetics, identification of risk factors for PONV related to patient characteristics, anesthesia, and surgery, and adherence to protocol-based prophylactic antiemetic use.
2.6. Apfel Risk Assessment
Based on the presence or absence of standard risk factors, such as female sex, non-smoking status, use of postoperative opioids, and history of PONV or motion sickness in the study population, the Apfel simplified risk score was calculated retrospectively. Patients were categorized as per their Apfel score to assess the relationship between baseline risk and PONV incidence.
2.7. Protocol Adherence Assessment
Adherence to institutional protocol-based prophylaxis was assessed by comparing the prophylactic antiemetic regimen used in the study population against the institutional protocol-based prophylaxis recommendations.
2.8. Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD). Comparisons of continuous variables between patients with and without PONV were performed using the Mann–Whitney U test. Categorical variables were presented as frequencies and percentages [n (%)]. The relationship between categorical variables and the incidence of PONV was assessed using the Chi-square test. The association between PONV incidence and adherence to institutional policy for perioperative antiemetic prophylaxis was also evaluated using the Chi-square test. All analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY), and p-values of <0.05 were considered statistically significant. A multivariable penalized logistic regression model was constructed to identify independent predictors of PONV.
3. RESULTS
3.1. Incidence of PONV
A total of 1113 adult patients who underwent inpatient surgery under general anesthesia were included in the final analysis. The mean (± SD) age of the study population was 40.6 ± 14.9 years, and 59.0% patients were female. Of 1113 patients, 199 developed PONV, yielding a PONV incidence of 17.9%.
3.2. Patient Demographic and Clinical Factors Associated with PONV
Patients who developed PONV were significantly older than those who did not have PONV (p=0.005). Baseline demographic and perioperative characteristics of patients with and without PONV are summarized in Table 1. Increasing ASA category was significantly associated with a higher incidence of PONV (p<0.001), with the highest incidence of PONV observed in ASA ≥IV. The mean Apfel score was significantly higher in patients with PONV than those without PONV (p=0.032).
| Variables | Patients without PONV (n=914) | Patients with PONV (n=199) | P-value |
|---|---|---|---|
| Age (years) (mean ± SD) |
39.9 ± 14.5 | 43.6 ± 16.4 | 0.005 |
| Female (%) | 524 (79.8%) | 133 (20.2%) | 0.017 |
| Male (%) | 390 (85.5%) | 66 (14.5%) | |
| BMI (kg/m2) | 29.1 ± 6.8 | 29.2 ± 7.6 | 0.621 |
| BMI category, n (%) | |||
| <25 | 234 (25.6%) | 51 (25.6%) | 0.717 |
| 25–29.9 | 257 (28.1%) | 48 (24.1%) | |
| ≥30 | 320 (35.0%) | 60 (30.2%) | |
| ASA score | 2.2 ± 0.8 | 2.6 ± 0.9 | <0.001 |
| ASA category, n (%) | |||
| ASA I | 134 (14.7%) | 17 (8.5%) | <0.001 |
| ASA II | 493 (53.9%) | 85 (42.7%) | |
| ASA III | 244 (26.7%) | 70 (35.2%) | |
| ASA ≥IV | 43 (4.7%) | 27 (13.6%) | |
| Apfel score | 2.39 ± 0.7 | 2.51 ± 0.7 | 0.032 |
| Apfel score ≥3, n (%) | 486 (53.2%) | 118 (59.3%) | 0.135 |
Abbreviations: SD – standard deviation; BMI – body mass index; ASA -American Society of Anaesthesiologists Physical Status Classification; PONV – post-operative nausea and vomiting.
3.3. Anesthesia-related Factors Associated with PONV
Mean duration of anesthesia was 131.5 ± 82.6 minutes overall and was significantly longer in patients with PONV than those without PONV (p=0.002) (Table 2). Anesthesia duration exceeding 5 hours was also significantly associated with PONV (p=0.018). The mean PACU length of stay in the overall study population was 40.5 ± 25.3 minutes. There was no significant difference in the PACU length of stay between patients with PONV and without PONV (p=0.126).
| Variables | Patients without PONV (n=914) | Patients with PONV (n=199) | P-value |
|---|---|---|---|
| Duration of anesthesia (minutes) (mean ± SD) | 127.8 ± 77.7 | 148.4 ± 100.6 | 0.002 |
| Duration of anesthesia >5 hours | 29 (3.2%) | 14 (7.0%) | 0.018 |
| PACU length of stay (minutes) (mean ± SD) | 40.8 ± 25.7 | 38.8 ± 23.1 | 0.126 |
Abbreviations: SD – standard deviation; PONV – post-operative nausea and vomiting, PACU - post-anesthesia care unit.
Desflurane was the most commonly used volatile anaesthetic, administered to 813 patients (73.1%), whereas sevoflurane was administered to 300 patients (27.0%). Out of 813 patients who received desflurane, 146 patients (18.0%) developed PONV, whereas out of 300 patients who received sevoflurane, 53 patients (17.7%) experienced PONV. This incidence of PONV in desflurane and sevoflurane groups was comparable with no statistically significant association (p=0.980). Propofol infusion was administered to all included patients (n=1113) as part of the anaesthetic technique. Among these patients, 199 (17.9%) developed PONV (Fig. 1). As all patients received propofol infusion, no comparative analysis could be performed to assess the relationship between propofol infusion use and the incidence of PONV.
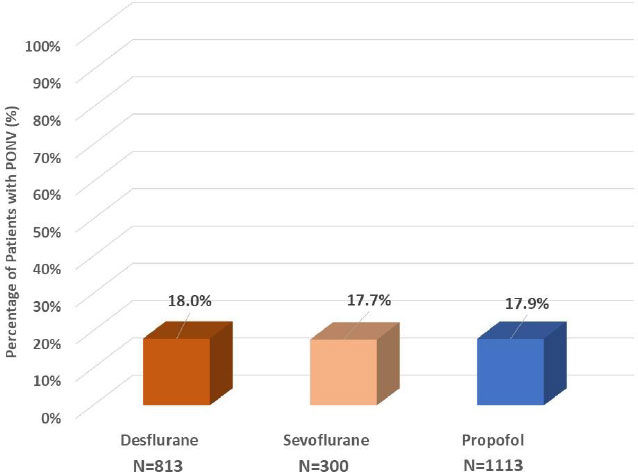
Postoperative nausea and vomiting across different anesthetic techniques.
3.4. Association between type of Surgery and PONV
As shown in Fig. (2), the type of surgery was significantly associated with PONV (p<0.001). The highest incidence of PONV was observed in patients who underwent renal surgeries (39.3%), followed by patients with gastrointestinal surgeries (26.3%). Patients who underwent gynaecological surgeries demonstrated the lowest incidence of PONV (5.5%).
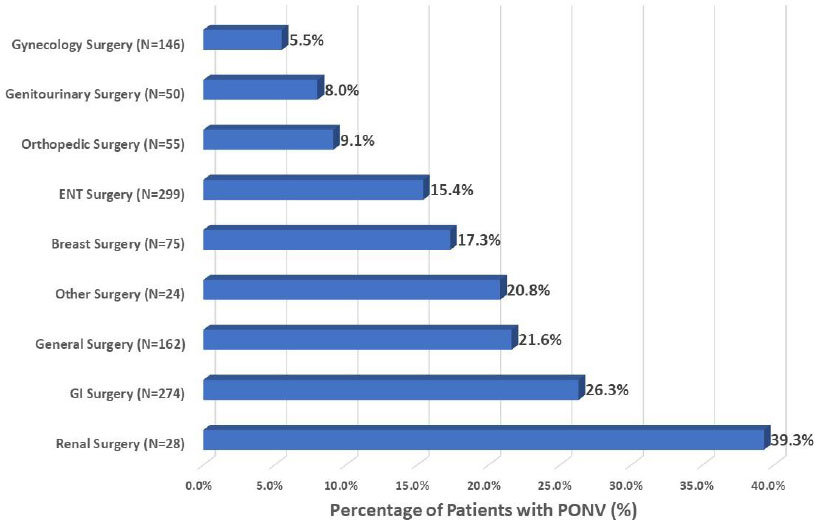
Postoperative nausea and vomiting across different surgical categories.
Abbreviations: ENT- Ear, Nose, Throat; GI – Gastrointestinal.
General surgery includes procedures such as incision and drainage of skin and soft tissue abscesses, biopsy or excision of lymph nodes, wound debridement, incision and drainage of anal abscess, and inguinal hernia repair (open or laparoscopic mesh repair).
3.5. Prophylactic Antiemetic use and Incidence of PONV
Preoperative antiemetics were administered to 151 (13.6%) patients, and 962 (86.4%) patients did not receive any preoperative antiemetic prophylaxis. Out of 151 patients who received preoperative antiemetics, 146 patients also received antiemetics intraoperatively. The incidence of PONV was numerically lower in patients who received preoperative antiemetics than in those who did not (16.6% vs 18.1%). However, this difference was not statistically significant (p=0.732) (Fig. 3). Intraoperative antiemetics were administered to 1062 patients (95.4%), and they had a significantly lower incidence of PONV than patients who did not receive any intraoperative antiemetics (16.9% vs 39.2%; p<0.001).
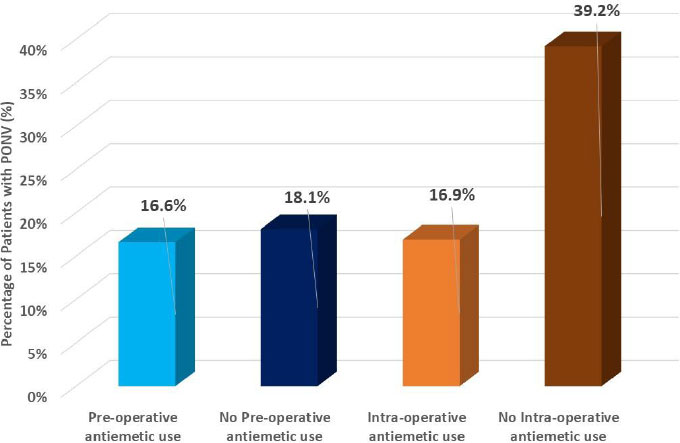
Efficacy of preoperative and intraoperative antiemetic prophylaxis in preventing PONV.
When prophylactic antiemetic use was analysed irrespective of timing of administration (i.e., preoperative and/or intraoperative), the majority of these patients (1062 of 1113; 95.4%) received at least one prophylactic antiemetic during the perioperative period, and 51 patients (4.6%) did not receive any prophylactic antiemetic at any time. Among patients who received any prophylactic antiemetic (preoperative and/or intraoperative), 180 patients (16.9%) developed PONV. In contrast, among patients who did not receive any prophylactic antiemetic, 20 patients (39.2%) experienced PONV. Overall, there was a significantly lower incidence of PONV in patients who received prophylactic antiemetics compared with those who did not (16.9% vs 39.2%; p<0.001).
3.6. Postoperative Antiemetic Administration
Out of 1113 patients, postoperative antiemetics were administered to 79 (7.1%). Out of 199 patients who developed PONV, 66 patients (33.2%) received postoperative antiemetics. Postoperative antiemetic use was significantly more common in patients with PONV than in those without PONV (33.2% vs 1.4%; p<0.001).
3.7. Commonly used Antiemetics and Relationship with PONV
Among patients who received preoperative antiemetics (n=151), the most frequently used antiemetic was metoclopramide, followed by ondansetron and dexamethasone, either as single agents or in combination (Table 3). In the intraoperative period, the most commonly administered antiemetics were ondansetron and dexamethasone, frequently combined. In the postoperative period, metoclopramide and ondansetron were the most commonly used rescue antiemetics. Intraoperatively, dual combination antiemetics were given to 823 (77.4%) patients, and triple combination antiemetics were given to 39 (3.7%) patients. Preoperatively, only 1 patient received a dual antiemetic combination; the rest (n=150) received a single antiemetic drug. Patients who did not receive any intraoperative antiemetic had the highest incidence of PONV (39.2%), whereas patients who received dual-agent antiemetic prophylaxis had the lowest incidence (16.2%; p<0.001). Triple-agent prophylaxis demonstrated a PONV incidence of 17.9%, similar to that seen with dual antiemetic therapy. Also, there was a statistically significant difference in the incidence of PONV across various intraoperative antiemetic combination regimens (p=0.0039). Patients who received combinations of ondansetron and dexamethasone had lower PONV incidence than those who received no antiemetic prophylaxis.
| Antiemetics Usage | Metoclopramide, n (%) | Ondansetron, n (%) | Dexamethasone, n (%) |
|---|---|---|---|
| Preoperative Antiemetics | 105 (69.5%) | 5 (3.3%) | 3 (2.0%) |
| Incidence of PONV | 12 (11.4%) | 2 (40%) | 2 (66.7%) |
| Intraoperative Antiemetics usage | 60 (0.6%) | 974 (91.7%) | 929 (87.5% |
| Incidence of PONV | 10 (16.7%) | 159 (16.3%) | 157 (16.9%) |
| Postoperative Antiemetics* | 51(64.6%) | 21 (26.6%) | 0 (0%) |
Note: *used as rescue antiemetics. The numbers presented for each antiemetic represent their use either as a single agent or in combination with other antiemetic agents. Therefore, the total percentage may exceed 100%.
3.8. Multivariable Analysis
A multivariable analysis was performed to identify independent predictors of PONV, including age, sex, BMI, ASA physical status, duration of anesthesia, Apfel score, perioperative prophylactic antiemetic use, and type of volatile anaesthetic used. In the adjusted analysis (Table 4; Fig. 4), female sex and a higher Apfel score were independently associated with higher odds of PONV. Age, BMI, ASA score, and duration of anesthesia were not statistically significant independent predictors of PONV. The use of perioperative prophylactic antiemetics (preoperative and/or intraoperative) was associated with lower odds of PONV, though this did not reach statistical significance. Similarly, volatile anaesthetic type was not independently associated with PONV.
| Variable | Adjusted OR (aOR) | 95% Confidence Interval | p-value |
|---|---|---|---|
| Female sex (vs male) | 1.5 | 1.1 – 2.1 | 0.025 |
| Apfel score (per 1-point increase) | 1.2 | 1.0 – 1.6 | 0.048 |
| Age (per 1-year increase) | 1.0 | 1.0 – 1.0 | 0.412 |
| Body mass index (per kg/m2) | 1.0 | 1.0 – 1.1 | 0.621 |
| ASA physical status (per 1-point increase) | 1.1 | 0.9 – 1.4 | 0.342 |
| Duration of anesthesia (per minute) | 1.0 | 1.0 – 1.0 | 0.286 |
| Any perioperative antiemetic prophylaxis (Yes vs No) | 0.6 | 0.3 – 1.4 | 0.263 |
| Desflurane vs sevoflurane | 0.9 | 0.6 – 1.3 | 0.395 |
Abbreviations: BMI – body mass index; ASA -American Society of Anaesthesiologists Physical Status Classification; CI – confidence interval, OR – Odds ratio.
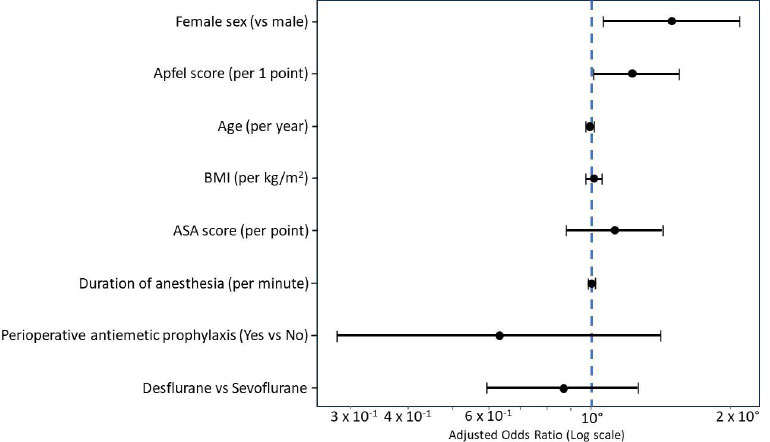
Forest plot of adjusted predictors of postoperative nausea and vomiting.
Abbreviations: Footnote: BMI – body mass index; ASA -American Society of Anaesthesiologists Physical Status Classification.
3.9. Adherence to Hospital Policy for Intraoperative Antiemetic Prophylaxis
The institutional hospital policy recommends the routine intraoperative administration of two antiemetics, dexamethasone and ondansetron, intravenously to all patients undergoing surgery under general anesthesia. In this study, 1062 patients (95.4%) received intraoperative antiemetics, suggesting high overall adherence to intraoperative prophylaxis recommendations. A total of 974 patients (91.7%) received ondansetron intraoperatively, while dexamethasone was administered to 929 (87.5%).
However, despite high usage of individual antiemetic agents, complete adherence to the hospital policy was not universal. 75.8% patients received dual antiemetic prophylaxis with dexamethasone and ondansetron intraoperatively. A smaller proportion of patients received single-agent prophylaxis, particularly in patients with diabetes due to concerns related to perioperative hyperglycaemia, while others received alternative antiemetic combinations or no intraoperative antiemetic at all. Patients who did not receive intraoperative antiemetic prophylaxis (n=51) had a significantly higher incidence of PONV than those who did (39.2% vs 16.9%; p<0.001), emphasizing the clinical relevance of adherence to policy-based antiemetic prophylaxis.
4. DISCUSSION
In this large retrospective cohort analysis, the overall incidence of PONV was 17.9%. Female sex, higher ASA physical status, longer duration of anesthesia, and higher Apfel scores were significantly associated with an increased risk of PONV. Overall, use of prophylactic perioperative antiemetic was associated with a significantly lower incidence of PONV compared with no prophylaxis (16.9% vs 39.2%, p<0.001). Furthermore, intraoperative prophylactic antiemetic use was also associated with a significantly lower incidence of PONV, with dual-agent antiemetic prophylaxis associated with the lowest incidence. The type of surgery also influenced the incidence of PONV, whereas the type of volatile anaesthetic was not associated with significant differences in PONV incidence. Notably, incomplete adherence to the institutional dual-agent prophylaxis policy highlights a gap between recommended anaesthetic practice and real-world implementation.
The observed PONV incidence of 17.9% in the present study falls within the lower range of incidence reported in other large observational and interventional studies (20–30%) [10, 13]. In a retrospective cohort study, Dash et al. reported a PONV incidence of 30.8% [14]. Similarly, a meta-analysis by Amirshahi M et al. reported an overall PONV prevalence of 27.7% [13]. Near-universal use of perioperative antiemetic prophylaxis, as per institutional policy requirements, may explain the relatively lower incidence of PONV observed in our study.
Among various perioperative factors related to risk of PONV, female sex emerged as a significant risk factor for PONV in our study, as highlighted in other prior studies [10, 15]. Apfel et al. (1999) reported female sex as one of the strongest independent predictors of PONV [10]. Apart from this, higher ASA physical status was significantly associated with an increased risk of PONV in our cohort. Even though the ASA score is not an element of the Apfel risk score, available data suggest a higher risk of PONV in patients who have multiple comorbidities, which may result in more complicated surgeries, requiring a longer duration of anesthesia and possibly higher usage of opioids [10, 16].
The important findings of this study, demonstrating a statistically significant association between higher Apfel scores and PONV, are well supported by previous studies showing a proportional increase in the risk of PONV with higher Apfel scores [10, 17]. The high risk of PONV associated with longer duration of anesthesia observed in our study is consistent with previous evidence [8, 10, 18]. Also, the significant association between surgery type and PONV risk observed in the current study is corroborated by previous studies, which showed variability in PONV risk across surgical types, particularly in abdominal and visceral procedures [11, 19].
Propofol-based anesthesia is well documented to be associated with a lower risk of PONV compared with volatile anaesthetic–based techniques [20]. This is partly attributed to the fact that propofol has inherent antiemetic properties, exerted via modulation of central dopaminergic pathways, inhibition of serotonin (5-HT3) receptor activity, and reduced activation of the chemoreceptor trigger zone [21]. As propofol was used in all included patients in our study, this might have partly contributed to the lower risk of PONV compared to the higher incidences observed in previous studies. Interestingly, the combined analysis of perioperative antiemetic use (preoperative and intraoperative) showed a significantly lower incidence of PONV in patients who received perioperative prophylactic antiemetics compared to those who received no antiemetic prophylaxis, strongly supporting the distinct effectiveness of perioperative prophylaxis strategies as a whole [22-24].
The adjusted multivariable analysis depicted female sex and higher Apfel score as independent predictors of PONV, highlighting the fundamental role of well-known patient-related risk factors in shaping the overall risk of PONV in surgical patients. The emergence of the Apfel score as an independent predictor of PONV despite widespread use of prophylactic antiemetics probably suggests that baseline PONV risk is a key driver of the occurrence of PONV in real-world practice. Although partial adherence to the hospital’s dual-agent intraoperative antiemetic prophylaxis recommendations was observed, the higher incidence of PONV in patients who did not receive intraoperative antiemetics reinforces the clinical importance of consistent protocol adherence. This emphasises the need for continuous education and quality-improvement initiatives.
Institutional management of PONV is based on a risk-stratified, multimodal approach. Patients need to be assessed preoperatively using the simplified Apfel score. Strategies to reduce baseline risk include the use of regional anesthesia whenever feasible, propofol-based anesthesia (including total intravenous anesthesia when appropriate), minimization of perioperative opioid use, and maintenance of adequate hydration. The pharmacological prophylaxis typically consists of intravenous dexamethasone (4–8 mg) administered at induction and intravenous ondansetron (8 mg) administered at the end of surgery, with combination therapy preferred over monotherapy. In selected cases, intravenous metoclopramide 10 mg can be used as an additional agent. Also, for patients who develop PONV, rescue antiemetic therapy should be administered using intravenous metoclopramide 10 mg.
5. CLINICAL RELEVANCE
Our study emphasizes that PONV is a common multifactorial post-operative complication in patients undergoing general anesthesia despite widespread use of prophylactic antiemetics. Although guidelines-recommended use of intra-operative prophylaxis significantly reduces the incidence of PONV, it does not completely eliminate the risk as various patient-, surgery-, and anesthesia-related factors independently influence the occurrence of PONV.
6. STUDY LIMITATIONS
Observations from a large real-world cohort of adult surgical patients included in this study enhance the generalizability of the findings to routine anaesthetic practice. However, this study has several limitations inherent to its retrospective observational study design. There also exists the possibility of bias in documenting the exact occurrence of PONV, particularly in patients with mild or transient symptoms. Furthermore, being a single-centre study, varying institutional practices may limit extrapolation to other settings with different anaesthetic or prophylactic protocols.
CONCLUSION
Despite widespread use of prophylactic antiemetics, the overall incidence of PONV was 17.9%. Female sex, higher ASA physical status, longer duration of anesthesia, and higher Apfel scores were significant determinants of PONV risk. Intraoperative prophylactic antiemetic administration, as recommended by institutional policy, was significantly associated with a reduced risk of PONV. The findings of this study reinforce the importance of consistent adherence to protocol-based, multimodal intra-operative prophylaxis and ongoing clinical audit to further reduce the burden of PONV and improve postoperative recovery.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: J.A.S.: Conceptualized and designed the study, supervised data collection, and critically revised the manuscript; J.A.K.: Contributed to study design, data acquisition, and interpretation of results; S.J.: Performed data analysis and statistical interpretation and contributed to drafting the Results section; A.K.: Assisted with data extraction, literature review, and preparation of tables and figures; R.E.D.: Contributed to the interpretation of findings and critically reviewed the manuscript for important intellectual content; K.S.A.: Assisted in manuscript drafting and editing and ensured adherence to reporting guidelines; G.K.C.: Provided overall supervision, reviewed the final manuscript, and approved the version for publication. All authors contributed to manuscript revision, read, and approved the final version, and agree to be accountable for all aspects of the work.
LIST OF ABBREVIATIONS
| SD | = Standard deviation |
| PACU | = Post-anesthesia care unit |
| PONV | = Postoperative nausea and vomiting |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Institutional Review Board, Dubai Hospital, Dubai, UAE (IRB approval number: MBRU IRB-2025-539, dated 4 June 2025).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
The requirement for informed consent was waived due to retrospective nature of the study and use of anonymized data.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this study were obtained from the institutional clinical database and are not publicly available due to institutional policy and patient confidentiality restrictions. De-identified data may be made available from the corresponding author upon reasonable request and subject to institutional approval.
ACKNOWLEDGEMENTS
The authors would like to thank the Head of the Department of Anesthesiology and the Quality team at Dubai Hospital for their support in data retrieval from the institutional electronic clinical database. They also acknowledge the contributions of the nursing staff in the post-anesthesia care unit and surgical wards for their meticulous documentation of postoperative outcomes, which made this study possible.

